Welcome back to The Sunday Morning Post. The goal of TSMP is that every post violates the rules of the news cycle by sharing stories from science, health, and history that will be as relevant in 10 years as in 10 hours.
Consider the number: 40,000. That’s about how many American men die each year from prostate cancer. It’s how many women die each year from breast cancer. Influenza killed about 40,000 Americans last year. So did Parkinson’s disease.
Imagine a biotech company announced that it had developed a vaccine that, if scaled nationally, could reduce the mortality rate of all these illnesses—prostate cancer, breast cancer, influenza, and Parkinson’s disease—by 90 percent. I think we’d call it a miracle drug.
The number, again: 40,000. It’s also how many Americans die each year from “traffic fatalities,” according to the US Department of Transportation. Car accidents are one of the most significant reasons for America’s unusually short lifespans. Men in the U.S. die more than 5 years younger than those in Japan or Switzerland, and auto accidents account for 10 percent of this expectancy shortfall—more than diabetes, cancer, or suicide, according to a 2022 analysis by the USC researcher Jessica Ho. Imagine, again, if some tech company announced that it had developed a product that, scaled nationally, could reduce the mortality rate of car accidents by 90 percent. I would like to think that we would consider it an absolute miracle.
Except, it exists. It’s Waymo—a driverless taxi service originally developed inside Alphabet, the parent company of Google. Studies evaluating tens of millions of miles driven by Waymo have found that, compared with human-driven vehicles, the company’s cars are involved in 96 percent fewer vehicle-to-vehicle crashes at intersections; 90 percent fewer bodily-injury claims; 92 percent fewer pedestrian injuries; and 88 percent fewer property damage claims.

So, why are so many progressive cities trying to prohibit Waymo cars, as if they were fentanyl on wheels? Timothy Lee writes that a number of Democratic-leaning states “are considering proposals to restrict or ban the deployment of driverless vehicles.” In a recent hearing before the Boston City Council, City Councilor Julia Mejia declared her “strong opposition” to Waymo cars; City Councilor Benjamin Weber found it “concerning to hear that the company was making a detailed map of our city streets without having a community process beforehand” (sorry, what?); and City Councilor Erin Murphy announced legislation requiring that a “human safety operator is physically present” in all driverless cars, which would make the current offering from Waymo technically illegal.
Feel the irony: Partisans blocking a healthy, life-saving technological invention due to fanatical precautions about unintended effects. These Democrats are the mirror image of vaccine-skeptic conservatives who stand athwart progress yelling stop in the realm of therapeutics. If anti-vax Republicans are turning into the party that hates medical progress for tribal reasons (e.g., a toxically conspiratorial attitude toward everything), anti-Waymo Democrats are in danger of becoming the party that hates software progress for their own clichéd reasons (e.g., a toxically cautionary approach to any change involving the physical environment). I do not want a world where life-saving vaccines are banned in red states while life-saving driverless cars are banned in blue states.
Driverless technology is growing fast, with monthly passenger miles growing by 700 percent in the last year. Still, Waymo is the epitome of the famous William Gibson observation that the future is here, but unevenly distributed. In a handful of cities like Phoenix and San Francisco, self-driving cars are everywhere, but in most cities, you cannot find a single Waymo car on the road. It will be a strange future indeed if, as Lee writes, “robotaxis are ubiquitous in cities like Miami, Atlanta, Dallas, and Houston [while] roads in Boston, Chicago, and Seattle look about the same in 2035 as they did in 2025.”
. The image is licensed under CC BY.")
The New York Times is the latest major news organization to ask: Why Are More Young People Getting Cancer? According to the National Cancer Institute, more than a dozen cancers increased in frequency among people under 50 in the U.S. between 2010 and 2019.
The journalist, Nina Agrawal, names some familiar suspects (e.g., obesity, poor diet, forever chemicals) and some I’d never heard of before. For example, I did not know that girls get their periods earlier than they used to, and, as women have children later, if at all, the resulting increase in menstrual cycles might create more rounds of cellular division in breasts, which raises the likelihood of more cancerous mutations.
But is the early-onset cancer epidemic real, or is it part of the phenomenon I described in my essay “The Age of Diagnosis”: Better technology and broader definitions of illness have led to an era where every condition seems to be an epidemic these days—not only psychological conditions, such as anxiety and depression, but also physical and neurological conditions, such as autism and PTSD. What is happening here is complicated. Many of us are more anxious, depressed, distracted, and sick. But we’re also testing ourselves more frequently for more loosely defined sicknesses, so the scale of each epidemic is, at the very least, exaggerated by diagnostic inflation.
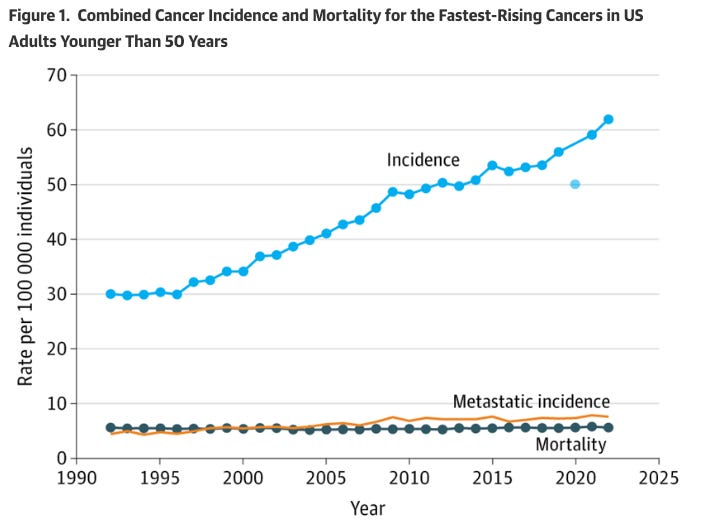
Perhaps, I’ve wondered, a similar thing is happening with early-onset cancers. Maybe some cancers really are becoming more frequent, but the general trend is being inflated by much more testing, more scanning, and more probing. If, for example, there were strong evidence that certain cancer diagnoses were rising while deaths for that cancer were flat or declining, that would be consistent with a story that doctors are detecting a lot of non-symptomatic cysts and calling it “cancer” even though there’s no underlying harm of out-of-control cellular division.
That’s precisely the conclusion of a new JAMA paper: “The Rise in Early-Onset Cancer in the US Population—More Apparent Than Real.” In the last 30 years, the number of early-onset cancers detected and diagnosed has soared, while the mortality rate for most of those cancers has not budged. Since the 1990s, the early-onset incidence for many cancers has doubled, while their early-onset mortality has remained “remarkably stable,” with the rate in 2022 identical to that in 1992.
Take thyroid cancer, for example:
Since 1992, more than 200,000 additional young women and men received diagnoses of thyroid cancer, while the number of deaths has remained virtually unchanged. Furthermore, there have been more than 100,000 additional diagnoses of melanoma and breast cancer, despite declines in deaths of each.
There are two big exceptions to this theory of over-detection and over-diagnosis. Colorectal and endometrial cancer are both seeing rising incidence and rising mortality, which suggests that these cancers really are becoming more frequent among young people. But overall, “the rise in early-onset cancer appears to be less an epidemic of disease and more an epidemic of diagnosis,” the authors write.
There is an existential tradeoff at the center of the age of diagnosis. We may live longer if we think of ourselves as permanent patients who must test ourselves constantly and neurotically for signs of disease. But we might not live better if we subject ourselves to a battery of infinite tests that frequently detects false signals of our eventual demise. Many of us will die of cancer. Also, many of us will die with dozens of weird growths and cysts inside of our bodies that have nothing to do with our ultimate cause of death. I don’t know that I want to know about, and worry about, every little bump in my body on the tiny chance that it saves me some minuscule amount of life. As the age of detection and diagnosis expands, people will face a legitimate choice with some hard questions. How much medical imagery is too much? How many scans are too many? Where is the line between protecting our bodies from premature demise and infecting ourselves with a new form of general anxiety?
Source link

