Happy Monday! Time to buckle up for another week (yes, that’s the pep talk I give myself every Monday).
Covid-19 levels may have peaked, but the messy ACIP vaccine headlines haven’t. This week will bring new headlines too, with RFK Jr.’s promised autism report expected to surface—I’ll get you ready for that. Plus: why falls among older adults are rising, and why loneliness is climbing among young people. Finally, a question from the YLE community about accessing Covid-19 vaccines at pharmacies.
Plenty to cover, but all tied back to what it means for you.
Join me today for a YLE webinar: All About Fall Vaccines. We’ll dive into the who, what, when, and where of flu, RSV, and Covid vaccines with Chelsea Cipriano from the Common Health Coalition. We’ve set aside 30 minutes to answer your questions live, too!
-
10am PT / 1pm ET
-
Paid subscribers can register here.
-
If you can’t make it this time, I will be sure to share the recording!
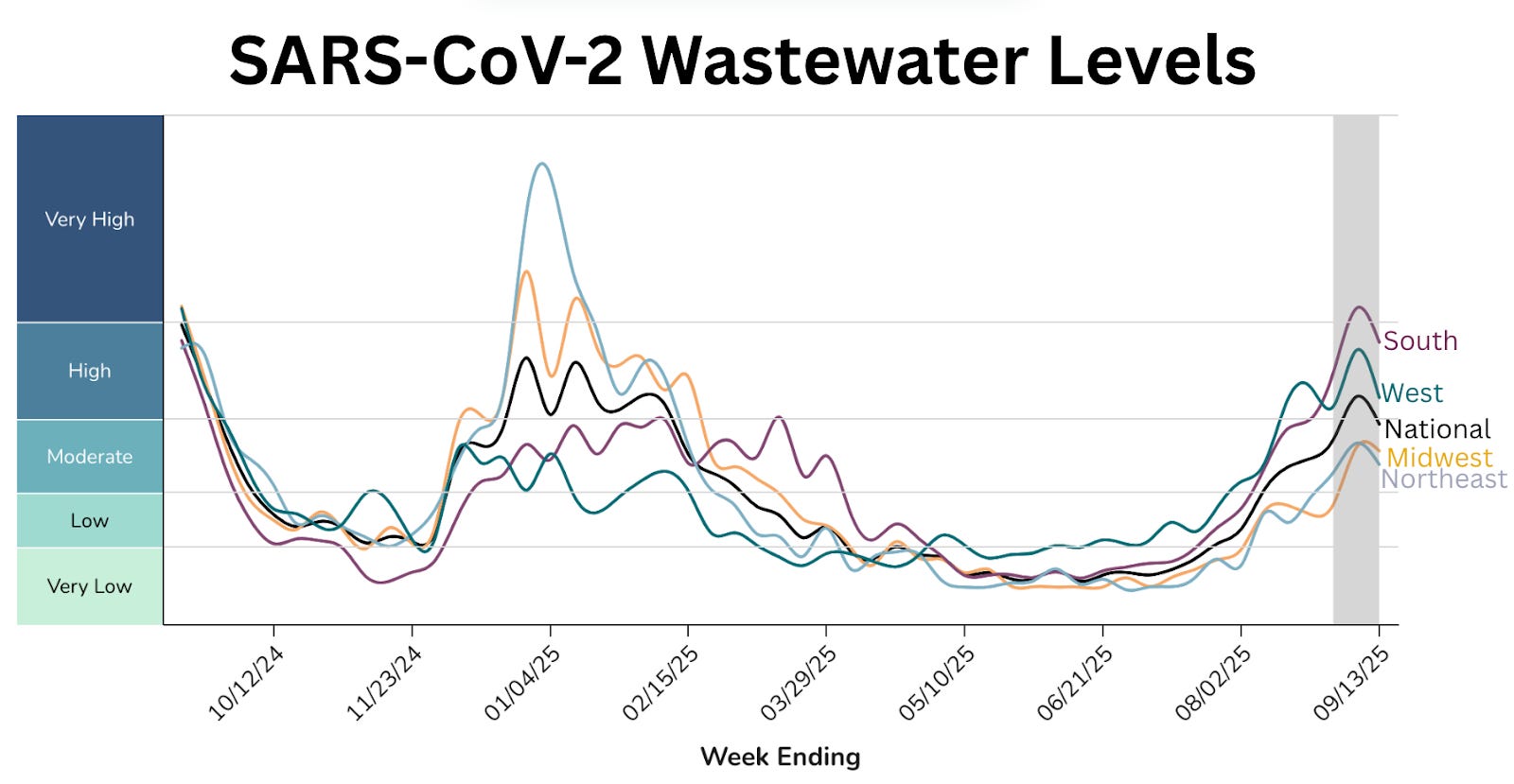
Covid-19’s summer wave has peaked. Wastewater, ER visits, and positive tests are all declining across the country. This surge was about the same size as last winter’s, but smaller than last summer’s, largely because no dramatically new variant emerged. The virus is still mutating, but in small steps rather than big leaps. We’ll see what this winter has in store when Covid waves usually begin in mid-November.
RSV and flu: Not too much stirring, yet.
Rhinovirus and enterovirus—also known as the common cold (gray line below)— continue to climb. In other words, there are a whole lot of people with stuffy noses and feeling crappy right now.
What does it mean for you? If you’re sick right now, it’s probably still Covid-19 or the common cold. When should you get your vaccines? Catch the breakdown here. Also, here’s how (and how not to) boost your immune system backed by science.
One of the quickest ways to drive down vaccine uptake is through confusing—or flat-out wrong—headlines. Especially now that we are all living headline to headline, trying to keep up with the firehose.
I was disappointed in the coverage following last week’s coverage of ACIP’s. Headlines were confusing and, at times, plain incorrect. I hope the media steps up; this won’t be the last vaccine rodeo.
Let’s be clear: Covid-19 vaccines are still recommended for everyone over 6 months of age—even by RFK Jr.’s handpicked ACIP members. (Surprising, yes, but likely a product of political and grassroots pushback. Still, we’ll take the win. Go here for my thoughts.)
-
Broad recommendation: The CDC still recommends vaccines for everyone 6 months and older under “shared clinical decision making.” This is broader than FDA’s approach (which excludes off-label use), but narrower than some professional organizations.
-
Insurance coverage: Vaccines remain covered across private plans, Medicaid, CHIP, and Medicare—no cost-sharing. Health insurance groups (AHIP, ACHP) affirmed they’ll continue coverage.
-
Pharmacy access: Pharmacists can counsel and vaccinate under shared decision making in all 50 states, which matters since >90% of adults get Covid vaccines in pharmacies.
Potential barriers to keep in mind:
-
Provider knowledge: Some providers, like pharmacists, aren’t yet familiar with shared decision making. It requires both education and time, which are already in short supply. Fair reimbursement for vaccine counseling could help.
-
Healthcare access: Not everyone has a provider to discuss vaccines or insurance coverage with.
-
Prescription rules: In some states, you may still need a prescription. Because vaccines are still considered off-label for some groups (like healthy adults and children, due to CDC and FDA misalignment), some states require prescriptions at pharmacies.
-
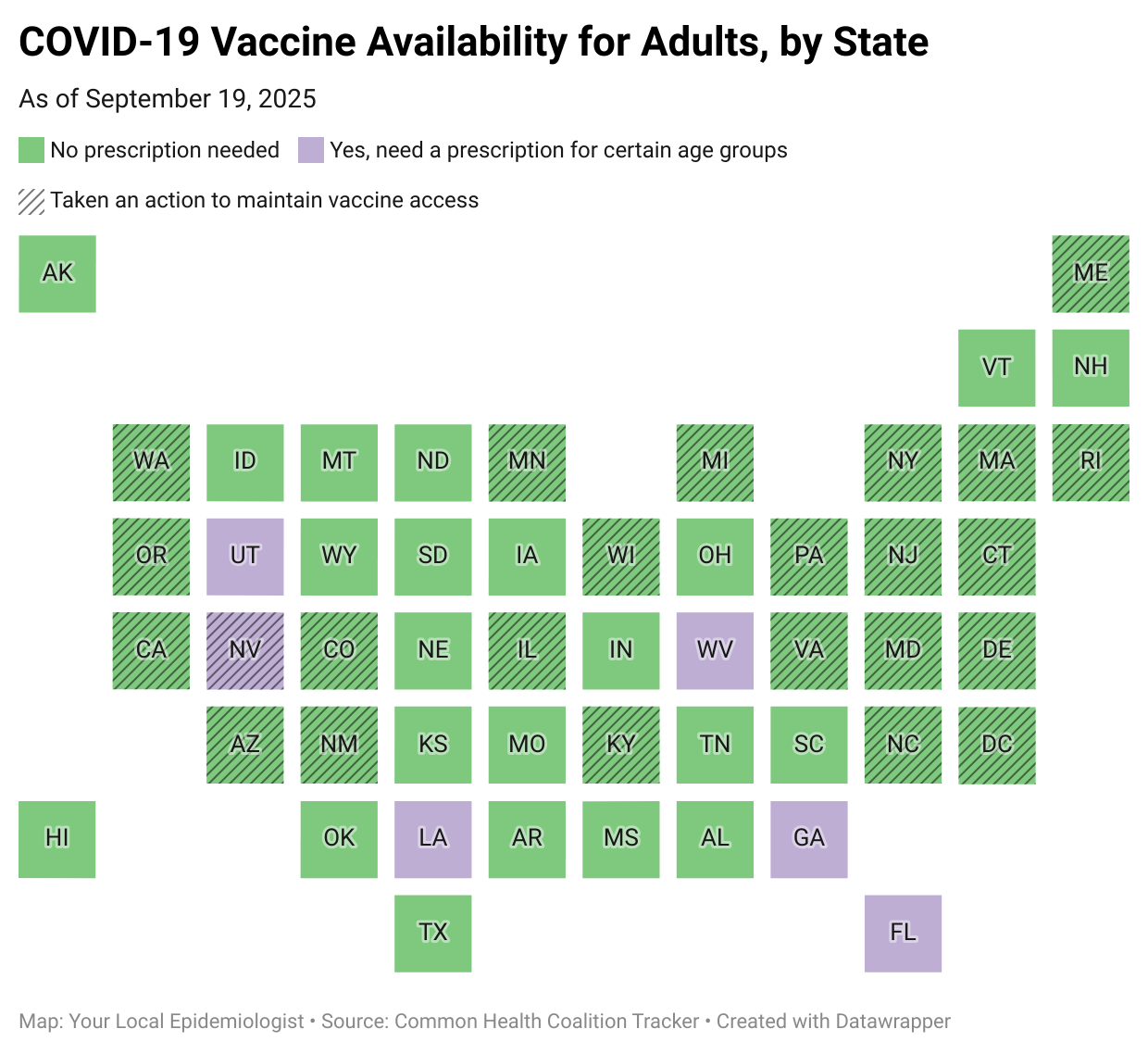
The good news: More than 23 states have “decoupled” from federal rules.
-
The bad news: Utah, Nevada, West Virginia, Louisiana, Georgia, and Florida still haven’t.
-
What does this mean to you? Get vaccinated.
Remember RFK Jr.’s promise to “find the cause of autism” by September? Well, it’s September. Word is his report is coming today (or this week). So consider this your prep.
Scientists have been studying autism for years by looking at genetics, environmental exposures, and other factors. Revisit the YLE post below for more.
I imagine he will do with this report what he does best: Mix kernels of truth with outright falsehoods. Word is that the report will cover the following (and likely more). Some quick nuance for you:
-
Tylenol during pregnancy. Early studies hinted at a possible correlation. But this was largely put to rest after a major 2024 study compared siblings—one exposed to Tylenol in utero, the other not. This “natural experiment” took into account genetics and family environment, and the result was clear: the link disappeared. There’s some data to suggest that fevers during pregnancy are linked to autism, which Tylenol can help prevent. Check out a deep dive here.
-
Folic acid during pregnancy. Large studies show folic acid is important for preventing serious conditions like neural tube defects. A few small studies have explored whether very high levels might shape development differently, but the evidence isn’t consistent. Check out a deep dive here.
-
Leucovorin: A treatment? A rare condition called cerebral folate deficiency, where folate in the blood looks normal but the brain doesn’t get enough, has been associated with developmental differences. In children who are both autistic and have this condition, leucovorin (folinic acid) has been studied in small trials. Some studies suggest possible benefits for communication and behavior, but much more research is needed. Be wary of anyone telling you to run out and buy this.
-
Vaccines. Over 25 epidemiological studies, including a fantastic 2019 analysis of more than 600,000 children in Denmark, have refuted any link.
One of the most harmful things this report could do is blame mothers and burden families with unfounded guilt. Autism is not something to “cure”—it’s a natural part of human diversity. People with autism deserve understanding, respect, inclusion, and the supports they need.
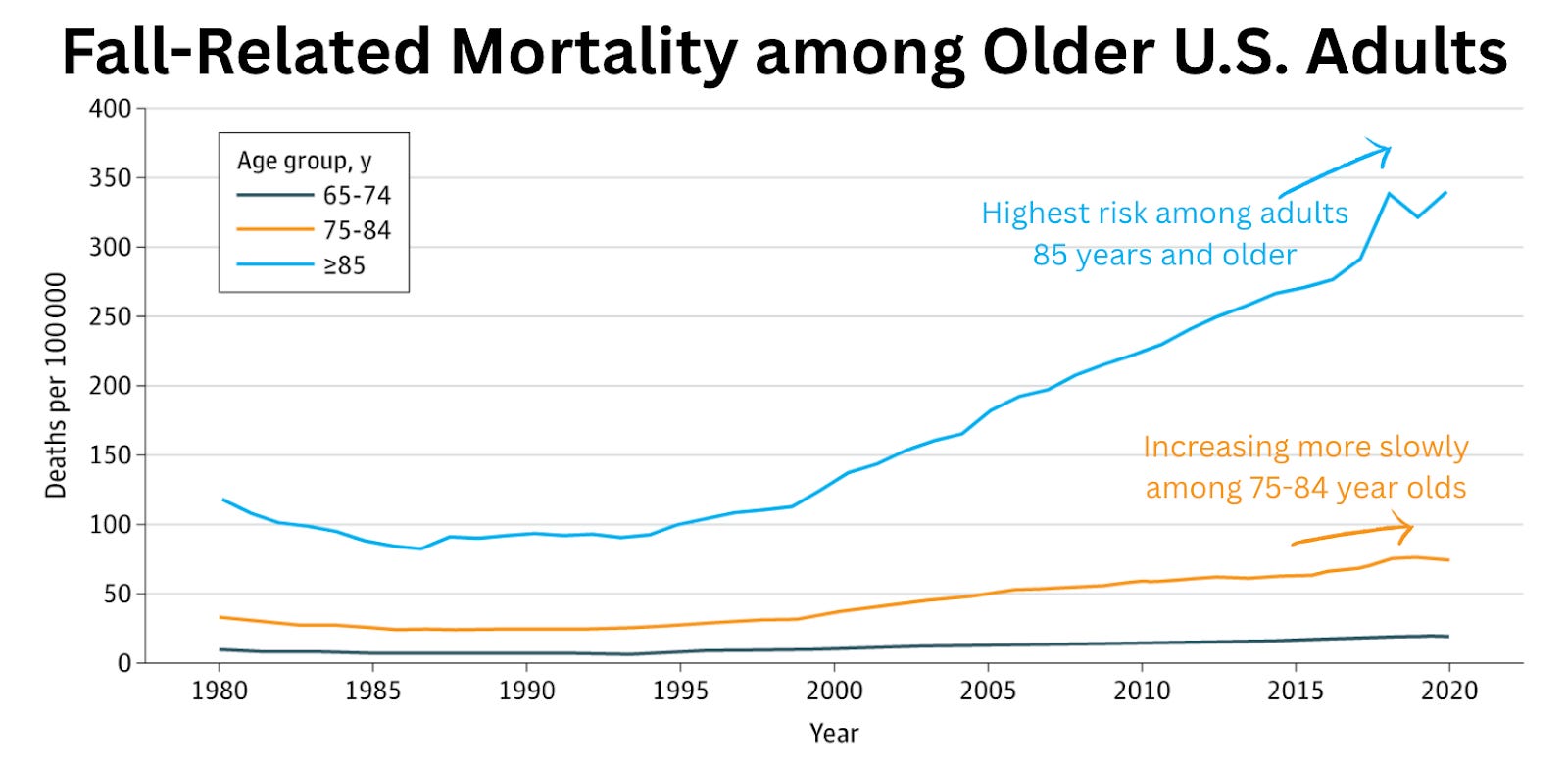
A recent review by Dr. Thomas Farley highlighted that, among those over 65, fall-related deaths have more than tripled over the past thirty years. Over 85 is the highest risk group. This now surpasses deaths from cancer, car crashes, and overdoses.
There are a few potential explanations for this:
-
Prescription trends: Many older adults are increasingly prescribed fall risk–increasing drugs (FRIDs), which are medications that can cause dizziness, drowsiness, or loss of balance. These include opioids, benzodiazepines, gabapentinoids, and some antidepressants prescribed, despite safer alternatives, at rising rates despite warnings from geriatric experts.
-
Reporting changes: Death certificates increasingly list falls as the cause of death.
-
Frailty: Today’s oldest-old are living longer but often with more comorbidities, making them more vulnerable.
What does it mean for you? If you’re older or caring for someone who is, review your medications with a doctor. Ask specifically about FRIDs.
Younger people are lonelier.
Two new polls reveal that 1 in 2 teenagers and young adults (13–24-year-olds) cite loneliness as the most common reason for disruptions in their daily lives, followed by family issues.
What does it mean for you? Connection matters. Encourage downtime, in-person friendships, and supportive online spaces. Communities protect against loneliness and other health risks.
So what does shared clinical decision making mean in practice when I go into Walgreens to get my COVID shot this fall? Just give my age (over 80) and that’s my “go-home-free” card? Or do I have to say “Yeah, I talked to my doctor about it and s/he said it’s a good idea” (whether or not that actually happened)? Or actually produce something in writing from a doctor?
Great question! In most cases, you’ll go up to the counter or schedule an appointment, just like you usually would.
-
If you’re in a green state (see figure above), you don’t need a doctor’s note or anything in writing.
-
If you’re in a purple state and considered “off-label” (like healthy adults under 65), you will need a prescription. Pharmacists can administer the vaccine, but they can’t write the prescription themselves.
So what does shared clinical decision making actually mean in practice? At its core, it’s a conversation about the benefits and risks of vaccines. That’s always been important, but how it’s carried out is left to the practitioner, and it can look different depending on where you go. Importantly, all pharmacists in all 50 states can do “shared clinical decision making” with you. Some pharmacists may use a standard template, while others will sit down for a one-on-one discussion. In some cases, a technician will cover the basics before the pharmacist gives final approval.
However it unfolds, expect it to take a little more time than usual, but the end result should be the same: you’ll walk away vaccinated.
Stay healthy and sane this week. Hope to see you at the webinar soon!
Love, YLE
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. YLE is a public health newsletter that reaches over 380,000 people in more than 132 countries, with one goal: to translate the ever-evolving public health science so that people are well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members. To support the effort, subscribe or upgrade below:
Source link


